anorexia and bulimia nervosa
- related: Psychiatry
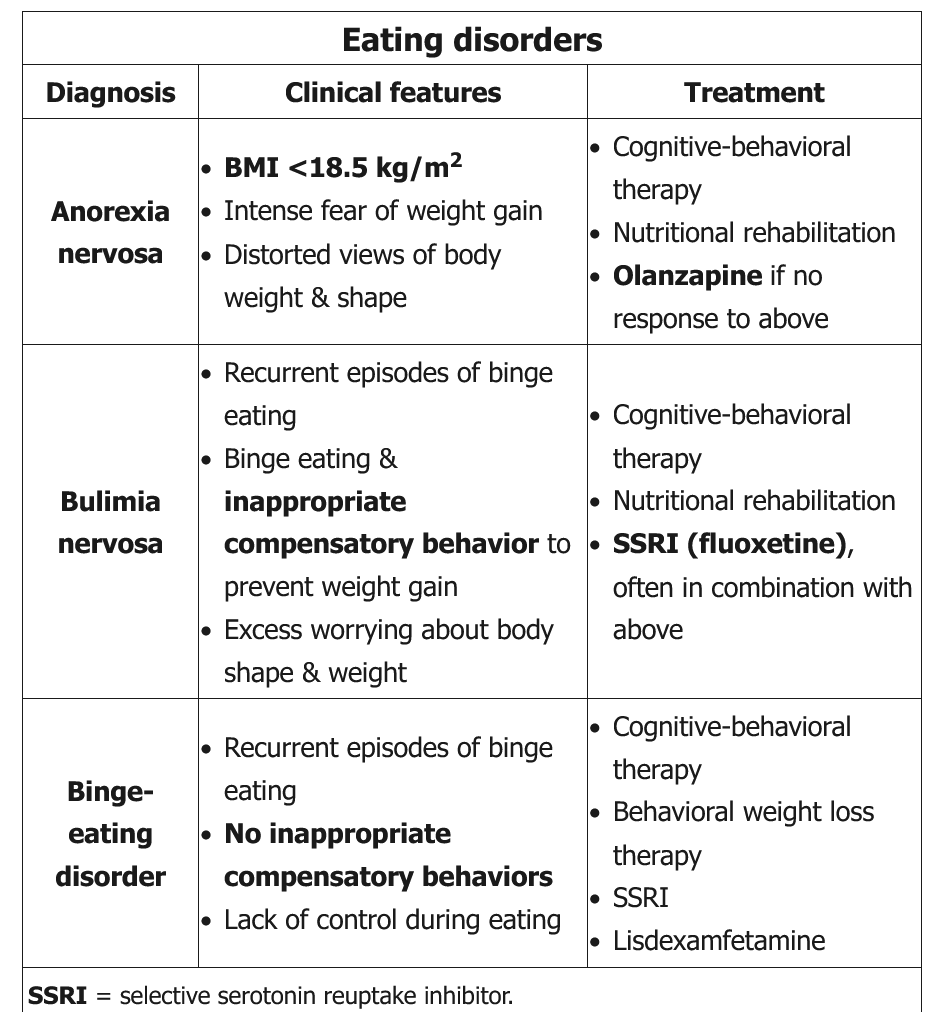
Self-induced vomiting is the most common compensatory behavior in bulimia nervosa and may cause electrolyte abnormalities (eg, hypokalemia, hypochloremia, metabolic alkalosis), erosion of dental enamel, and parotid hypertrophy. However, some patients engage in misuse of laxatives, enemas, diuretics, diet pills, fasting, or excessive exercise to control their weight. Binge-eating disorder also involves repetitive episodes of binge eating but does not include the inappropriate compensatory behaviors seen in bulimia nervosa (Choice C).
First-line treatment for anorexia nervosa (AN) involves psychotherapy and nutritional rehabilitation (establishing a structured and consistent meal pattern). Pharmacotherapy is not an initial or primary treatment of AN and is generally used as an adjunct in treatment-resistant cases.
Although several types of psychotherapy have been used to treat AN, cognitive-behavioral therapy (CBT) is commonly recommended and is supported by multiple guidelines. CBT focuses on the dysfunctional thoughts (eg, negative self-evaluation based on weight and shape) and behaviors (excessive food restriction) that maintain the disorder. It is a structured and time-limited therapy that includes self-monitoring and homework between sessions. Family therapy is also effective and is particularly recommended for adolescents.